Acute otitis media


Acute otitis media (or AOM, the inflammation of the middle ear, or middle ear infection) is an illness caused by viruses or bacteria, which develops as a complication following an infection of the upper respiratory system.
It can occur in patients of any age but is most common in young children, with those between 3 months and 3 years of age at greatest risk..
Development and causes:
< AOM is most often preceded by a catarrhal illness of viral origin of the upper respiratory system.
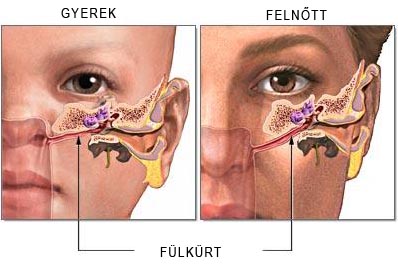
swelling of the mucous tissue closes the opening of the Eustachian tube, which normally ventilates the middle ear.
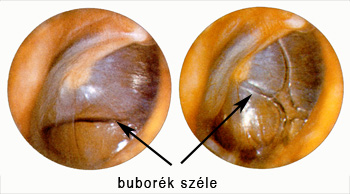
The Eustachian tube is normally ventilated 3 to 4 times minute during swallowing. In case of an inflammation, the Eustachian tube cannot ventilate, the air inside is absorbed, and serous discharge accumulates in its place behind the eardrum. This condition is known as serous inflammation of the middle ear.. fü
fülviszketés füldugulás víz a fülben gyulladás viszketés
If the serous discharge is superinfected, it provides conditions for bacteria to multiply.
Infections get into the middle ear space and purulent otitis develops.

The infection can get in through the Eustachian tube (most common), through the blood stream, as well as from the outside as a result of the rupture or perforation of the eardrum which, in turn, can be the result of water reaching it, from the bath water or from ear washing, or the result of incautious removal of a foreign object from the outer auditory path.
 Viruses can prepare the way for bacterial superinfection as well.
Viruses can prepare the way for bacterial superinfection as well.
Usually the mucous tissue of the tympanic cavity as well as that of the bone behind the ear is infected, causing mastoiditis to develop concurrently to AOM
Besides catarrhal illnesses of the upper respiratory system, other conditions such as adenoids, allergic conditions and the reflux disease (or Gastro-Esophageal Reflux Disease or GERD) can increase susceptibility to the recurrent development of AOM.
A dysfunction of the ventilation of the middle ear and sinuses can also be caused by the acidification of the body.
Mucous tissues of the maxillary sinuses, Eustachian tube and the middle ear tend to swell and produce abnormal mucus during detoxification processes, since the body attempts to withdraw through the mucus the superfluous acids and toxins produced by the body when attempting to bind acids.
Symptoms and diagnostics:

In its early stages the illness produces few symptoms, however, an otological examination can reveal the retraction of the eardrum and a better visibility of its blood vessels.
Classic symptoms of inflammation occur during the course of the disease: swelling, hyperemia, pain, and dysfunction.
Persistent and strong earache is a typical symptom of purulent otitis. Infants often reach for their ears and cry out in pain. Older patients may report a loss of hearing as well. General symptoms include high fever, faintness, and despondency.
Complaints and symptoms vary according to the phase of the disease:
Complaints and symptoms vary according to the phase of the disease:
 First phase:
First phase:
Inflammation with a discharge for 1-2 days, a temperature of 39-40 ºC (102-104 ºF), in more severe cases shivering, pain and stiffness in the nape in children.
Elderly patients often do not develop fever. Other symptoms are strong, pulsating pain, which is stronger at night than during the day, a sensitivity of the mastoid are to pressure, a dull ringing in the ears occurring synchronically to the pulse, and a loss of hearing.

Second phase:
Delimitation (3-8 days): The eardrum usually ruptures, discharging pus from the ear, eliminating the pain and the fever.
This phase can be shortened significantly by administering antibiotics at the beginning of the treatment, averting the rupture of the eardrum as well.
Third phase:
Recovery (2-4 weeks): discharge from the ear gradually subsides, and hearing is restored.
 In young children vomiting and diarrhea may occur due to the fact that the pus dripping down the esophagus may irritate the gastrointestinal system.
In young children vomiting and diarrhea may occur due to the fact that the pus dripping down the esophagus may irritate the gastrointestinal system.
Consecutive dehydration aggravates symptoms further. If proper otological treatment is delayed, the eardrum ruptures.
This alleviates pain, since pressure on the eardrum decreases. The drainage through the ruptured eardrum is bloody and has pus in it.
Diagnostics:

First phase:
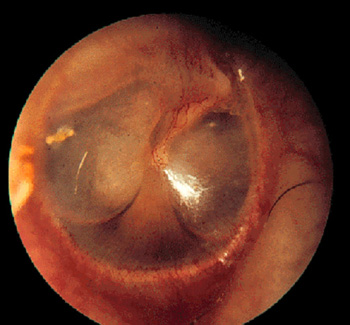
Microscopic image: The eardrum is sanguine, the blood vessels dilate. The eardrum thickens and loses its shine.
The contours of the handle and short appendage of the malleus disappear. At the height of the discharge phase the eardrum bulges forward, especially its postero-superior quadrant, and pulsation can be detected as well.
Infection can reach the outer auditory canal as well, in which case the borderline between the auditory canal and the eardrum disappears. Due to the concurrent mastoiditis, the mastoid area is sensitive to palpation. Conductive hearing impairment occurs.
 Second phase:
Second phase:
A tiny, needlepoint sized fistula forms usually in the postero-superior quadrant of the eardrum, through which pulsating non-smelling pus drains.
X-ray: the mastoid cells are opaque, no ostenecrosis occurs, i.e. the bone edges are sharp.
Third phase:
Pulsation stops, the quantity of the discharge decreases and becomes glassy and mucous, and finally the discharge stops altogether. The eardrum thins out and is no longer sanguine, and anatomical structures are recognizable. The rupture of the eardrum heals spontaneously, leaving behind a small scar. Hearing is restored, and the cellular system gradually clears up.
Differential diagnosis
Inflammation of the outer auditory canal: The outer cartilage of the ear, the cartilage of the auditory canal is sensitive to pressure. Discharge drains without pulsation, is usually foul smelling and is never mucous. Little or no hearing impairment occurs. X-rays are negative.
Treatment
Middle ear infections require restoring the ventilation of the tympanic cavity and removing the discharge through the surgical procedure of myringotomy, during which a small incision is made on the eardrum with a lance shaped surgical tool and the pus is drained.
The procedure is usually carried out with a local anesthetic.
Sometimes the incision closes before full recovery is reached, which might require for myringotomy to be performed again. Waiting for the eardrum to rupture or perforate by itself is not recommended, since this leaves an irregularly shaped tear on the eardrum, which heals with difficulty and leaves a scar, ultimately causing permanent hearing impairment in some patients.
 Otological treatment might have to be accompanied by the administration of antibiotics for a minimum of 5 days and for 2-3 days after symptoms cease.
Otological treatment might have to be accompanied by the administration of antibiotics for a minimum of 5 days and for 2-3 days after symptoms cease.
Broad spectrum penicillin class antibiotics are recommended at first, with others to follow if necessary depending on the culture.
Recovery can be also aided by administering nose drops, fever reducers, pain relievers, as well as ear drops.
If recurring is caused by adenoids, removing the pharyngeal tonsils provides the permanent solution.
 In severe and recurring cases of middle ear infection in children a tympanostomy tube (or grommet) is inserted into the eardrum. Parents of young patients are necessary to inform about the dangers of non-surgical rupture, which usually inflicts greater damage than the surgical incision of the myringotomy.
In severe and recurring cases of middle ear infection in children a tympanostomy tube (or grommet) is inserted into the eardrum. Parents of young patients are necessary to inform about the dangers of non-surgical rupture, which usually inflicts greater damage than the surgical incision of the myringotomy.
The tube is a few millimeters in size and functions as a valve, allowing air to pass continuously from the tympanic cavity. It is removed after the critical stage of the disease is past.
Since the acidification of the body plays a great role in the development of the middle ear infection, a key element of the treatment might be detoxification and alkalizing the body, supplemented by a carefully controlled diet.
This can be accomplished easiest through taking natural alkalizing supplements.
The product recommended by us contains a unique mixture of 49 different organically grown vegetables, grasses, leaves and sprouted grains. It contains more than 125 natural vitamins, minerals and amino acid, which makes the maximal absorption of bases possible. It has an energizing effect and helps the oxygen intake of blood from water. It is a strong oxygen catalyst and helps the optimal functioning of body cells. It alkalinizes the body and reduces acid levels.
For more information.
With other questions, call at +36-20-397 4144 or send email to
Ez az e-mail-cím a szpemrobotok elleni védelem alatt áll. Megtekintéséhez engedélyeznie kell a JavaScript használatát.
About the product or order the product click here
Progress and prognosis:
 In the first, acute phase, early otological complications can develop depending on the intensity of the infection, the resistance of the body, and the effectiveness and suitability of the antibiotics.
In the first, acute phase, early otological complications can develop depending on the intensity of the infection, the resistance of the body, and the effectiveness and suitability of the antibiotics.
In the second phase, complications develop only rarely, but, as a result of insufficient antibiotic treatment, an increase in the resistance of the pathogens, or lack of the body’s resistance, a prolonged case of otitis and consecutive prolonged mastoiditis can develop.
In the third phase, in most cases a complete recovery from the acute otitis and the mastoiditis occurs. Late complications can occur about 2-3 weeks after the development of AOM, producing the following symptoms: recurring fever, recurring earache and discharge, an occurrence of headaches, a general deterioration of the patient’s state, and an increase in the drop of blood count levels.
The tasks of the family practitioner are as follows: refer child patients to a specialist, provide treatment in consultation with otolaryngology and pediatric specialists.
Prevention
 Since AOM develops as a result of infections of the upper respiratory system, the prevention of the development and proper treatment of the latter are the most important preventive measures.
Since AOM develops as a result of infections of the upper respiratory system, the prevention of the development and proper treatment of the latter are the most important preventive measures.
Vitamin rich diet is important in the fall and winter months. Nose drops can be helpful in the case of developed catarrhal diseases, while the removal of nasal discharge can help in children. Breathing through nose needs to be restored.
Removal of adenoids can be recommended in children, while in adults the surgical treatment of maxillary sinusitis, nasal polyps and septal deviation are recommended. Improperly treated AOM can result in hearing impairment, facial paralysis, cerebral abscess or meningitis.
 AOM in infants
AOM in infants
The younger the child, the greater the general symptoms and the more hidden the local signs, with gastrointestinal symptoms often becoming more prominent. Infants and young children are anatomically more prone to developing middle ear infections through the Eustachian tube, since their Eustachian tubes are short, straight and wide, the character of the mucous membrane of their middle ear and upper respiratory system is unified, they are susceptible to respiratory infections, their tonsillar rings are turgid, the canals of the middle ear are filled with swollen mucous membranes and are improperly ventilated.
Local symptoms
 Children frequently reach towards their ears, react with pain to pulling of and pressing on ears. The eardrum loses its glossiness, is grayish red, hardly bulging, but anatomical structures are unrecognizable.
Children frequently reach towards their ears, react with pain to pulling of and pressing on ears. The eardrum loses its glossiness, is grayish red, hardly bulging, but anatomical structures are unrecognizable.
Spontaneous rupture of the eardrum is rare, occurring in the antero-inferior quadrant. Discharging is also relatively rare (it drips down easily along the short, straight, and wide tube), but when it occurs, it is viscous, while pulsation is strong. Polyp formation sometimes occurs. Local lymphadenitis also occurs sometimes, the lymph nodes behind the ears swell.
Treatment:
Administering antibiotics is recommended. Nose drops are most effective in form of spray. Fever reduction and alleviation of pain as well as removing nasal discharge is necessary. A timely application of myringotomy is crucial, surgical opening of disease affected bone may be necessary. Surgery is recommended even if X-ray is negative, clinical symptoms are decisive.
Progress, prognosis:
The progression of the illness is prolonged, dramatic improvement often occurs only following surgery. In case of proper treatment the prognosis is good.
Actions required of family practitioner:
A seemingly unexplained lack of thriving or stalling of development in infants and young children mastoiditis needs to be tested for by a specialist. The treatment of the child is to be carried out by pediatrician and otolaryngologist together.
Back to the top
2007 © Studiomed Plusz Bt.
Találatok: 8125