Serosal otitis

An acute inflammation of the cavity system of the middle ear
Lat. otitis media serosa, otitis media acuta non suppurativa
 Serosal otitis is basically an illness caused by pathological discharge collected in the tympanic cavity without acute inflammation.
Serosal otitis is basically an illness caused by pathological discharge collected in the tympanic cavity without acute inflammation.
It occurs mostly in children, and its main symptom is conductive hearing impairment of up to 30 dB, discovered usually by audiology examination.
Its etiology is debated, but most likely multifunctional, with local and general immunological processes playing the most important role in both the development and thickening of the discharge. The process is dangerous due to the fact that without proper treatment it can lead to permanent hearing impairment.
History and symptoms:
Patients experience blunt hearing, fullness and pressure in the ear, and unpleasant popping at swallowing. If, in addition to fluid, air also gets into the tympanic cavity (e.g. at forced nose blowing), the splashing of the fluid can be heard at the movement of the head. Ache occurs occasionally.
Symptoms:
The illness usually occurs together with the catarrh of the upper respiratory system, and the symptoms of the two combine.
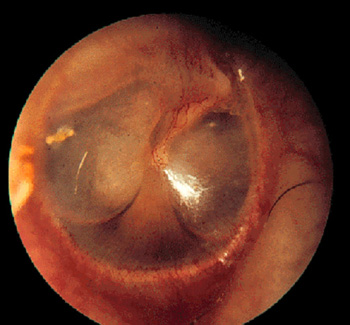
Microscope image: the eardrum is strongly retracted, the handle of malleus looks shortened, the short appendage of the malleus is more prominent. The cone of light is shortened or disappears.
 The flexible part of the eardrum (pars tensa) is amber colored and slightly grayish because of the translucent and first thin, later thickened fluid collecting behind it.
The flexible part of the eardrum (pars tensa) is amber colored and slightly grayish because of the translucent and first thin, later thickened fluid collecting behind it.
Sometimes the level of the fluid or air bubbles are visible in the fluid behind the eardrum. Conductive hearing impairment can be detected.
Course of the disease:
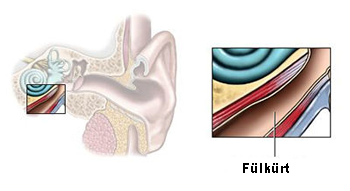
The malfunctioning of the Eustachian tube plays an important role, which can be caused by the following factors:
• Insufficiency of the muscle lifting the soft palate (m. tensor veli palatini).:
• A swelling of the mucous membrane of the Eustachian tube, caused by inflammation from neighboring areas (chronic maxillary sinusitis or adenoids), allergy, or a post-radiation state.
. 
• Adenoids can narrow the opening of the Eustachian tube mechanically as well.
• A factor increasing susceptibility to the illness could be the difficulty in the flow of the air stream due to deviation of the nasal septum.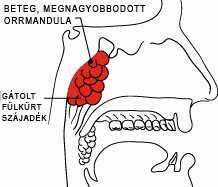
• Tumor in the nasopharynx.
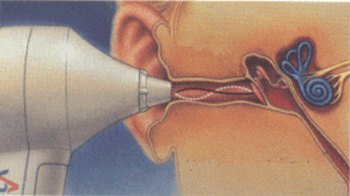
If the ventilation of the middle ear is partly or fully blocked, air is absorbed and negative pressure develops in the tympanic cavity.
The negative pressure irritates the mucous membrane of the middle ear, causing the following conditions:
o Edema occurs in the swollen mucous membrane
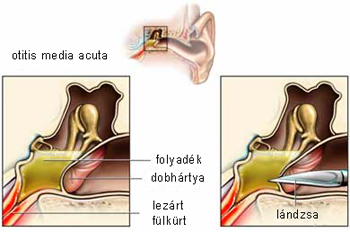
o Fluid collects (transsudatum) in the tympanic cavity
o The eardrum is retracted, the auditory ossicles become stiff
o The eardrum achieves a look of radiating vascularity.
o The eardrum ring bulks up
 Diagnosis:
Diagnosis:
The history is typical. Microscopic examination provides unambiguous images.
Conductive hearing impairment can be detected and measured in an audiology examination. A tympanometric examination can detect negative pressure in the tympanic cavity and show a typically flattened tympanogram.
Differential diagnosis
Signs are unambiguous, causes need to be discovered. Excluding the possibility of nasopharyngeal tumor is essential. Allergy may be possible cause.
Treatment:
Suspension of the causing factor is essential, possible ways: treatment of upper respiratory inflammation, adenotomy, treatment of allergy, correction of septal deviation, or radiation treatment for nasopharyngeal tumor.
Possible medications: salicylates, nose drops, antihistamines, and Calcium. Applying warmth locally or short wave treatment can help the excess fluid dissipate. Regular nose blowing is essential for restoring ventilation. Warmth can be applied to maxillary sinuses as well. Removal of adenoids and tonsils is warranted on the long run. Maxillary sinusitis, if occurs, should be properly treated.
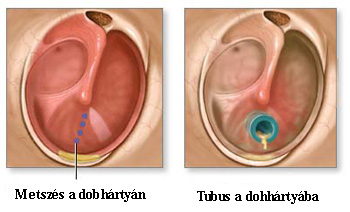 In protracted cases insertion of grommet (or tympanostomy tube) is advised.
In protracted cases insertion of grommet (or tympanostomy tube) is advised.
Progression and prognosis: usually good, but condition may become chronic.
Tasks of the family practitioner:
Treatment of condition together with catarrh of the upper respiratory system; chronic cases should be referred to a specialist.
Warning: In case of acute catarrh of the upper respiratory system permeability to the Eustachian tube should not be restored with Politzer’s or other methods because they can introduce pathogens to the middle ear and cause acute serosal middle ear infection to develop. The possibility of nasopharyngeal tumor has to be excluded.
Hits: 6830